Conservative treatment options:

Spinal problems do not always require surgery. Conservative treatments are the best way to address back pain. Spinal surgery can be delayed or eliminated in the vast majority of new neck and back injuries.
Physical therapy -is the best initial form of treatment in many cases after the initial injury to assess stable, non-emergent conditions. Neck and back injuries often require strengthening and re-education of the muscles around the spine to better support the spinal column.
Rehabilitation -is offered when the patient’s normal functional capacity is reduced after a back injury. The goal is to regain prior functional status in order to return to daily living and working abilities.
Strengthening -of the paraspinous muscles will help decrease repeat injury to the spine. Pilates or other forms of core body strengthening is often used to develop abdomen, thoracic and back (core) strength.
Intervertebral disc decompression (traction) therapy -is an option for acute and sub acute disc injuries. The system allows the disc some relief from the natural compression process while it is still in the healing phase.
Steroid injections - Injections into the symptomatic region such as epidural and selective nerve root blocks as well as other specialized injections are diagnostic and can also be therapeutic in many instances.
Medication - is an integral part of conservative treatment as it can help reduce the inflammatory process that leads to spasm, pain and further deterioration of the injured spine.
Physical therapy -is the best initial form of treatment in many cases after the initial injury to assess stable, non-emergent conditions. Neck and back injuries often require strengthening and re-education of the muscles around the spine to better support the spinal column.
Rehabilitation -is offered when the patient’s normal functional capacity is reduced after a back injury. The goal is to regain prior functional status in order to return to daily living and working abilities.
Strengthening -of the paraspinous muscles will help decrease repeat injury to the spine. Pilates or other forms of core body strengthening is often used to develop abdomen, thoracic and back (core) strength.
Intervertebral disc decompression (traction) therapy -is an option for acute and sub acute disc injuries. The system allows the disc some relief from the natural compression process while it is still in the healing phase.
Steroid injections - Injections into the symptomatic region such as epidural and selective nerve root blocks as well as other specialized injections are diagnostic and can also be therapeutic in many instances.
Medication - is an integral part of conservative treatment as it can help reduce the inflammatory process that leads to spasm, pain and further deterioration of the injured spine.
Surgical treatment options for stenosis:

Laminectomy/Laminoplasty – helps relieve pressure on the spinal cord by opening the spinal canal. The lamina which is the posterior roof of the spinal canal is either lifted or removed to create more space for the spinal cord and nerves. A fusion may be considered if stabilization is an issue.
Diskectomy – a common surgical procedure to treat the damaged discs by either removing the ruptured portion of the disc (microdiskectomy) in order to relieve the pressure on the nerve.
Vertebrectomy/Corpectomy – surgical removal of a portion of the vertebral body in the process of excising tumor, fractured bone, or infected bone imbedded in the vertebral body. A mechanism of support scaffolding is often used to stabilize the spine at this time.
Diskectomy – a common surgical procedure to treat the damaged discs by either removing the ruptured portion of the disc (microdiskectomy) in order to relieve the pressure on the nerve.
Vertebrectomy/Corpectomy – surgical removal of a portion of the vertebral body in the process of excising tumor, fractured bone, or infected bone imbedded in the vertebral body. A mechanism of support scaffolding is often used to stabilize the spine at this time.
Surgical treatment options for instability:
Spinal Fusion – is surgery that involves fusing adjacent vertebrae in order to stabilize the spine and reduce pain.
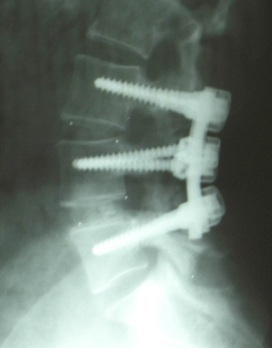
Posterior Fusion – approach to spinal fusion involves performing a partial diskectomy and often laminotomy followed by the placement pedicle screws inserted into the upper and lower vertebrae and connected with rods or plates.
Transforaminal Lumbar Interbody Fusion (TLIF) – is a lateral approach of the spine for placement of an intervertebral body spacer to fuse the adjacent vertebral bodies. Pedicle screws are inserted afterwards to help maintain stability.
Anterior Lumbar Interbody Fusion (ALIF) – approaches the vertebral bodies from the front through the abdomen. A metal plating system is placed to stabilize the spine while the intervertebral body spacer fuses the adjacent bodies.
Anterior/ Posterior (360) – is similar to an ALIF, but includes a posterior approach to secure the spine with pedicle screws and rod system.
Arthroplasty – Placement of artificial discs has been studied for years and recently one product has been approved by the FDA as an alternative to spinal fusion. Its believe that the benefits of artificial discs include, but not limited to preserving motion of the spine resulting in less restriction of motion and improved preservation of adjacent discs. The ADR is FDA approved for the lower back and at OMC ADR for the neck is being investigated currently.
Posterior Fusion – approach to spinal fusion involves performing a partial diskectomy and often laminotomy followed by the placement pedicle screws inserted into the upper and lower vertebrae and connected with rods or plates.
Transforaminal Lumbar Interbody Fusion (TLIF) – is a lateral approach of the spine for placement of an intervertebral body spacer to fuse the adjacent vertebral bodies. Pedicle screws are inserted afterwards to help maintain stability.
Anterior Lumbar Interbody Fusion (ALIF) – approaches the vertebral bodies from the front through the abdomen. A metal plating system is placed to stabilize the spine while the intervertebral body spacer fuses the adjacent bodies.
Anterior/ Posterior (360) – is similar to an ALIF, but includes a posterior approach to secure the spine with pedicle screws and rod system.
Arthroplasty – Placement of artificial discs has been studied for years and recently one product has been approved by the FDA as an alternative to spinal fusion. Its believe that the benefits of artificial discs include, but not limited to preserving motion of the spine resulting in less restriction of motion and improved preservation of adjacent discs. The ADR is FDA approved for the lower back and at OMC ADR for the neck is being investigated currently.
